The face and jaws change more from birth to age four than at any other period of development after birth. At birth, infants have no teeth and their skull bones have not yet fused, allowing rapid growth. This period has a strong influence on the development of the jaws and face. The majority of malocclusions are established by the end this stage of development. Birth is the point at which the infant begins using its jaws and facial musculature in earnest.
The development of the jaws and face is very plastic, particularly during this period. Genes do not determine the absolute size or shape of any body structure. Genes carry the blueprint for all structures, and influence their size and shape, but structures develop relative to one another and in response to the forces applied to them during growth. This is how orthodontists can change tooth alignment and occlusion by applying force to the teeth and jaws.
Influences on Early Postnatal Face and Jaw Development
In 1987, Miriam H. Labbok and colleagues published a subset of the results of the National Health Interview survey (now called NHANES) in the American Journal of Preventive Medicine. Their article was provocatively titled "Does Breast-feeding Protect Against Malocclusion"? The study examined the occlusion of nearly 10,000 children, and interviewed the parents to determine the duration of breast feeding. Here's what they found:
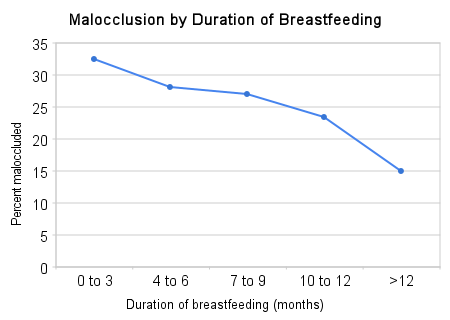 The longer the infants were breastfed, the lower their likelihood of major malocclusion. The longest category was "greater than 12 months", in which the prevalence of malocclusion was less than half that of infants who were breastfed for three months or less. Hunter-gatherers and other non-industrial populations typically breastfeed for 2-4 years, but this is rare in affluent nations. Only two percent of the mothers in this study breastfed for longer than one year.
The longer the infants were breastfed, the lower their likelihood of major malocclusion. The longest category was "greater than 12 months", in which the prevalence of malocclusion was less than half that of infants who were breastfed for three months or less. Hunter-gatherers and other non-industrial populations typically breastfeed for 2-4 years, but this is rare in affluent nations. Only two percent of the mothers in this study breastfed for longer than one year.The prevalence and duration of breastfeeding have increased dramatically in the US since the 1970s, with the prevalence doubling between 1970 and 1980 (NHANES). The prevalence of malocclusion in the US has decreased somewhat in the last half-century, but is still very common (NHANES).
Several, but not all studies have found that infants who were breastfed have a smaller risk of malocclusion later in life (1, 2, 3). However, what has been more consistent is the association between non-nutritive sucking and malocclusion. Non-nutritive sucking (NNS) is when a child sucks on an object without getting calories out of it. This includes pacifier sucking, which is strongly associated with malocclusion*, and finger sucking, which is also associated to a lesser degree.
The longer a child engages in NNS, the higher his or her risk of malocclusion. The following graph is based on data from a study of nearly 700 children in Iowa (free full text). It charts the prevalence of three types of malocclusion (anterior open bite, posterior crossbite and excessive overjet) broken down by the duration of the NNS habit:
 As you can see, there's a massive association. Children who sucked pacifiers or their fingers for more than four years had a 71 percent chance of having one of these three specific types of malocclusion, compared with 14 percent of children who sucked for less than a year. The association between NNS and malocclusion appeared after two years of NNS. Other studies have come to similar conclusions, including a 2006 literature review (1, 2, 3).
As you can see, there's a massive association. Children who sucked pacifiers or their fingers for more than four years had a 71 percent chance of having one of these three specific types of malocclusion, compared with 14 percent of children who sucked for less than a year. The association between NNS and malocclusion appeared after two years of NNS. Other studies have come to similar conclusions, including a 2006 literature review (1, 2, 3).Bottle feeding, as opposed to direct breast feeding, is also associated with a higher risk of malocclusion (1, 2). One of the most important functions of breast feeding may be to displace NNS and bottle feeding. Hunter-gatherers and non-industrial cultures breast fed their children on demand, typically for 2-4 years, in addition to giving them solid food.
In my opinion, it's likely that NNS beyond two years of age, and bottle feeding to a lesser extent, cause a large proportion of the malocclusions in modern societies. Pacifier use seems to be particularly problematic, and finger sucking to a lesser degree.
How Do Breastfeeding, Bottle Feeding and NNS Affect Occlusion?
Since jaw development is influenced by the forces applied to them, it makes sense that the type of feeding during this period could have a major impact on occlusion. Children who have a prolonged pacifier habit are at high risk for open bite, a type of malocclusion in which the incisors don't come together when the jaws are closed. You can see a picture here. The teeth and jaws mold to the shape of the pacifier over time. This is because the growth patterns of bones respond to the forces that are applied to them. I suspect this is true for other parts of the skeleton as well.
{kind=link}
Any force applied to the jaws that does not approximate the natural forces of breastfeeding or chewing and swallowing food, will put a child at risk of malocclusion during this period of his or her life. This includes NNS and bottle feeding. Pacifier sucking, finger sucking and bottle feeding promote patterns of muscular activity that result in weak jaw muscles and abnormal development of bony structures, whereas breastfeeding, chewing and swallowing strengthen jaw muscles and promote normal development (review article). This makes sense, because our species evolved in an environment where the breast and solid foods were the predominant objects that entered a child's mouth.
What Can We do About it?
In an ideal world (ideal for occlusion), mothers would breast feed on demand for 2-4 years, and introduce solid food about halfway through the first year, as our species has done since the beginning of time. For better or worse, we live in a different world than our ancestors, so this strategy will be difficult or impossible for many people. Are there any alternatives?
Parents like bottle feeding because it's convenient. Milk can be prepared in advance, the mother doesn't have to be present, feeding takes less time, and the parents can see exactly how much milk the child has consumed. One alternative to bottle feeding that's just as convenient is cup feeding. Cup feeding, as opposed to bottle feeding, promotes natural swallowing motions, which are important for correct development. The only study I found that examined the effect of cup feeding on occlusion found that cup-fed children developed fewer malocclusion and breathing problems than bottle-fed children.
Cup feeding has a long history of use. Several studies have found it to be safe and effective. It appears to be a good alternative to bottle feeding, that should not require any more time or effort.
What about pacifiers? Parents know that pacifiers make babies easier to manage, so they will be reluctant to give them up. Certain pacifier designs may be more detrimental than others. I came across the abstract of a study evaluating an "orthodontic pacifier" called the Dentistar, made by Novatex. The frequency of malocclusion was much lower in children who did not use a pacifier or used the Dentistar, than in those who used a more conventional pacifier. This study was funded by Novatex, but was conducted at Heinrich Heine University in Dusseldorf, Germany**. The pacifier has a spoon-like shape that allows normal tongue movement and exerts minimal pressure on the incisors. There may be other brands with a similar design.
The ideal is to avoid bottle feeding and pacifiers entirely. However, cup feeding and orthodontic pacifiers appear to be acceptable alternatives that minimize the risk of malocclusion during this critical developmental window.
* Particularly anterior open bite and posterior crossbite.
** I have no connection whatsoever to this company. I think the results of the trial are probably valid, but should be replicated.
No comments:
Post a Comment